Summary
- Many residency programs risk sanctions by unintentionally violating ACGME duty hour rules, which often stem from the complexities of manual scheduling.
- Common violations include miscalculating the 80-hour weekly average with moonlighting, misusing the 24+4 rule, and failing to protect the 14-hour post-call rest period.
- The root cause of most violations is treating compliance as a post-scheduling audit rather than a set of mathematical constraints that must be met from the start.
- Programs can prevent violations by building schedules with ACGME rules as unbreakable constraints; a managed service like Scheduling Wizard delivers mathematically optimized and compliant schedules without requiring programs to operate new software.
For many interns, averaging 88 hours per week isn't a bad week — it's just another Tuesday. And behind that number is a quiet, systemic fear: report it, and you'll be told to "manage your hours more efficiently." Stay silent, and the violations compound.
The stakes are real. If your program is found by the Accreditation Council for Graduate Medical Education (ACGME) to regularly be violating duty hours, it can be sanctioned — up to and including loss of accreditation. For program directors and chiefs, that's an existential threat.
Most violations aren't intentional. They're the product of a complex scheduling puzzle being solved manually, reactively, and under pressure. Before we get into the specific ACGME duty hour violations, here's a fast-read primer on the five rule categories every program must comply with.
The 5 Core ACGME Duty Hour Rule Categories (Quick Reference)
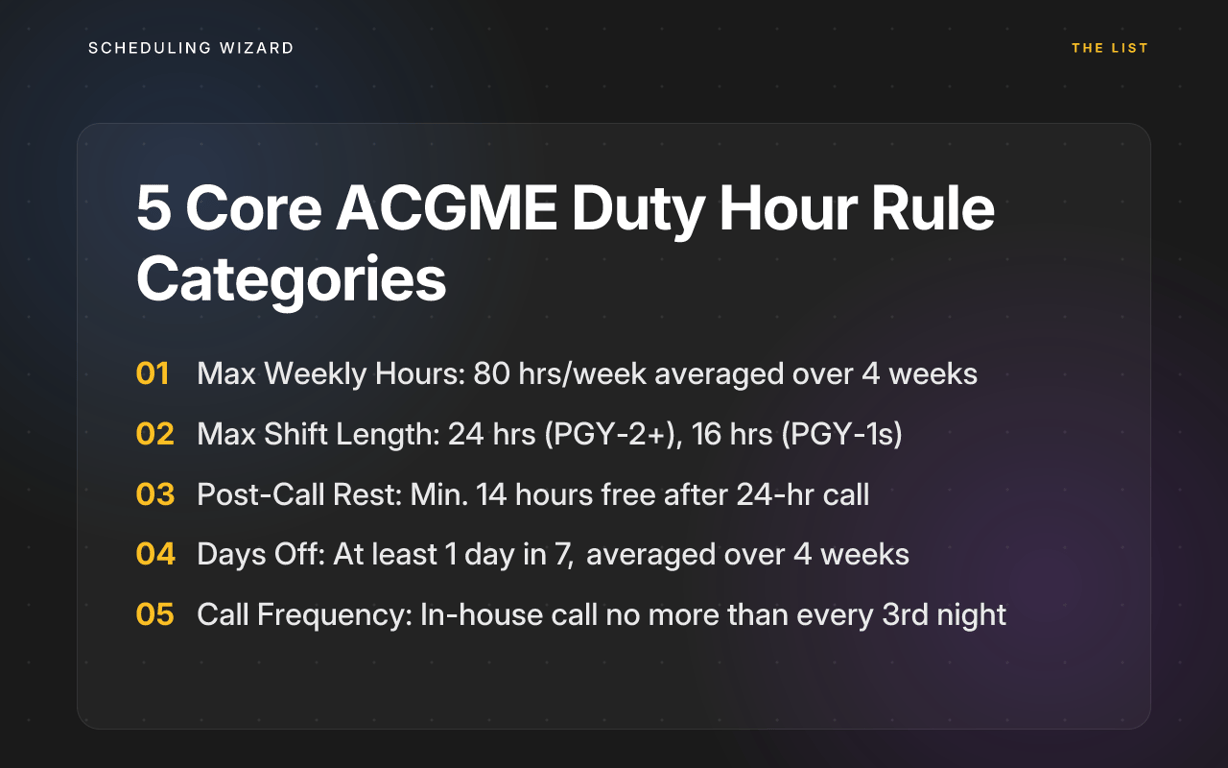
Per the ACGME Common Program Requirements:
| Rule | Requirement |
|---|---|
| Maximum Weekly Hours | 80 hours/week, averaged over 4 weeks — includes moonlighting |
| Maximum Shift Length | 24 hours continuous duty (PGY-2+); 16 hours max for PGY-1s |
| Post-Call Rest | Minimum 14 hours free after a 24-hour in-house call |
| Days Off | At least 1 day in 7, averaged over 4 weeks (4 days/28-day block) |
| Call Frequency | In-house call no more than every third night, averaged over 4 weeks |
Keep these in mind as you read each violation below — you'll see how easily one misstep cascades into another.
The 7 Most Common ACGME Duty Hour Violations
Each of these violations stems from a common root cause: treating compliance as an afterthought. Here are the seven most common ways programs fall out of compliance.
1. Exceeding the 80-Hour Weekly Limit When Moonlighting Is Factored In
Scheduling Wizard flags this before the schedule goes live. Most scheduling tools don't.
Here's a scenario that plays out often in surgical programs: a resident works 90 hours during a trauma week, 85 the following week, then 70 and 75 in lighter elective weeks. On paper, the four-week average looks like 80 hours — exactly at the cap.
But that resident also picked up two 8-hour moonlighting shifts during those lighter weeks. The real average: 84 hours. A clear violation.
What triggers it: Moonlighting hours — both internal and external — must be counted toward the 80-hour cap per ACGME requirements. Spreadsheet-based scheduling tools almost never include these. The chief resident is tracking institutional shifts, not total duty hours.
Most exposed specialties: General Surgery, Internal Medicine, Critical Care.
What compliant looks like: The schedule treats the 80-hour average as a hard mathematical constraint across the full four-week block, with moonlighting baked into the calculation — not tracked separately after the fact. Scheduling Wizard's proprietary optimization engine does exactly this: it models the entire block prospectively, accounts for all logged duty hours (including moonlighting preferences), and is designed to ensure the average never exceeds 80 hours before the schedule is ever published.
2. Misapplying the 24+4 Continuous Duty Rule
The 24+4 rule is arguably the most misunderstood rule in Graduate Medical Education (GME). And attendings sometimes exploit that ambiguity — intentionally or not.
The scenario: an internal medicine resident finishes a 24-hour call, completes signout, and is heading out. An attending asks them to "just see one more new admission." The resident, worried about a professionalism hit, stays. That's hour 26, and it involves new clinical responsibilities. Violation.
As residents on r/Residency describe it: "Programs abuse it to be 28hrs because they know you can't say no without getting hit with a professionalism violation."
What triggers it: The additional 4 hours are strictly for transitional care activities — completing handoffs and ensuring continuity for existing patients. No new admissions. No new procedures. The UW GME guidelines explicitly flag exceeding 28 consecutive hours as a reportable violation.
Most exposed specialties: General Surgery, Anesthesiology, Internal Medicine.
What compliant looks like: Clear institutional policy and attending-level education on what the +4 window covers. Schedules should have a hard stop at 24 hours for any new clinical work, with documented protection for the handoff window. For programs seeking a hands-off approach, compliance-focused scheduling services build these hard stops directly into their ACGME-compliant scheduling models from the start.
3. Breaking the 14-Hour Post-Call Rest Window
A family medicine resident finishes a 26-hour call at 9 AM Tuesday. Their next scheduled shift — a continuity clinic — starts at 7 AM Wednesday. That's 22 hours off: fine under the rules.
But then a co-resident calls in sick Tuesday afternoon, and the chief asks the post-call resident to cover a 4-hour evening shift starting at 6 PM. They returned to duty just 9 hours after finishing a 24+ hour call. Violation.
What triggers it: Unplanned absences with no protected backup coverage. When short-staffing happens, post-call residents are the most convenient — and the most dangerous — option to pull back in.
Most exposed specialties: Emergency Medicine, Family Medicine, Pediatrics.
What compliant looks like: The 14-hour post-call window must be treated as untouchable in the schedule — no clinical duties, no mandatory didactics, no coverage gap-filling. A true compliance-first system like Scheduling Wizard hard-blocks any attempt to schedule a post-call resident within this protected window, treating it as an unbreakable mathematical constraint.

4. The "1 Day Off in 7" Miscalculation
This one hides in plain sight. A pediatrics resident works 6 days, takes a 24-hour call on day 7 that ends the morning of day 8, then works days 9 through 13. The chief marks day 8 as a "day off" because the resident wasn't scheduled. But the resident was on-call through the night — that's not a day off. It's a post-call morning.
What triggers it: Two common misunderstandings: (1) treating the post-call morning as a free day, and (2) failing to track the four-week average rather than week-by-week compliance. A resident can work more than 6 consecutive days in some blocks — as long as 4 full, unencumbered calendar days are distributed across every 28-day period.
Most exposed specialties: Family Medicine, Pediatrics, any program running frequent call schedules.
What compliant looks like: Days off are tracked as a four-week rolling average, with the system distinguishing between post-call rest periods (which don't count) and true 24-hour duty-free days (which do). Four days per 28-day block is the minimum — and the schedule should enforce this at the point of construction.
5. Violating In-House Call Frequency (The Q3 Rule)
A resident goes on unexpected medical leave. To maintain coverage, the chief schedules the remaining residents Q2 for one week and Q3 for the remaining three. It feels like a temporary fix. But averaged across the month, the affected residents exceeded the every-third-night cap. Violation.
As one chief described the stress of this situation on r/Residency: "If vacations would otherwise force a pool into a week of Q2 call, I would rotate someone from a more senior pool into the rotation to break up the Q2." But sometimes, there's simply no one to rotate in.
What triggers it: Staffing gaps that tempt even well-intentioned chiefs into temporarily exceeding call frequency. Manual tools make it difficult to calculate the rolling four-week average across the entire resident pool in real time.
Most exposed specialties: Anesthesiology, Neurology, Orthopedic Surgery.
What compliant looks like: The scheduling system mathematically enforces the Q3 average across any 28-day window, flags the moment any individual falls below that threshold, and surfaces alternative coverage options before the violation is locked in.
6. Ignoring the 16-Hour Shift Cap for PGY-1s
A new chief resident inherits last year's call schedule template and assigns PGY-1s to the same 24-hour call slots as senior residents. The tool doesn't flag it. The first intern works a 24-hour shift on day one of the new academic year. Significant violation.
What triggers it: Generic scheduling tools or recycled templates with no differentiation between PGY levels. Chief resident turnover — the very problem Scheduling Wizard was built to solve — means this institutional knowledge frequently walks out the door every July.
Most exposed specialties: General Surgery, Internal Medicine, any program with mixed PGY-level call teams.
What compliant looks like: PGY-1 residents have a separate, hard-coded rule profile within the scheduling system. Their shifts are automatically capped at 16 hours with no manual override possible. This isn't a checkbox — it's a constraint baked into the schedule generation logic itself, as outlined in ACGME's requirements for first-year residents.
7. Treating Compliance as an Audit Instead of a Constraint
This is the meta-violation — and it's the root cause of most of the others.
The scenario: a chief builds the entire month's schedule, runs the compliance report, and gets back 15 violations. Now begins the painful process of manually untangling one constraint to fix another, often creating new violations in the process.
As one EM resident described their scheduling software experience: "The setup is tedious and error-prone." That frustration compounds when the errors have regulatory consequences.
A study published in PMC underscores a parallel issue: inaccurate resident logging creates reporting gaps that obscure how widespread violations actually are. The compliance problem is bigger than any single schedule.
What triggers it: Using scheduling tools that audit compliance after the schedule is built — rather than treating ACGME rules as mathematical constraints that shape the schedule from the start. Spreadsheet-based workflows compound the problem.
Most exposed specialties: All specialties, but especially those with complex multi-layered schedules like Surgery and Internal Medicine.
What compliant looks like: ACGME duty hour rules are hard constraints in the optimization model. The schedule cannot be generated in a violating state. There is no "run report and fix" cycle — compliance is the output, not a post-hoc check.
Stop Auditing. Start Preventing.
The common thread across every violation above isn't malice or indifference — it's a reactive system. Chief residents are solving complex constraint puzzles manually, under time pressure, with tools that weren't purpose-built for GME. And then they rotate out, taking all their institutional knowledge with them.
Manual audits after the schedule is built are a band-aid. They find violations after residents have been handed a problematic schedule. Real compliance means violations are impossible to schedule in the first place.
That's the difference Scheduling Wizard was built to deliver. Scheduling Wizard, backed by Y Combinator (YC W26), is a managed scheduling service — not another scheduling platform for your chief to learn. It's a done-for-you service: programs submit their constraints — rotations, call requirements, resident preferences, faculty availability, and all ACGME rules — and receive a finished, mathematically optimized, ACGME-compliant schedule delivered as an Excel file, ready to upload directly into Amion or QGenda.
The proprietary constraint-solving engine treats every ACGME duty hour rule as a hard mathematical requirement, not a post-build checklist item. PGY-1 caps, the 14-hour post-call window, moonlighting-inclusive 80-hour averages, Q3 call frequency — all of it is baked into the generation logic.
If a compliant schedule exists within your constraints, Scheduling Wizard finds it. The result is institutional scheduling continuity that doesn't depend on which chief resident happens to be in the seat this year.
Frequently Asked Questions
What is the most common ACGME duty hour violation?
Exceeding the 80-hour weekly limit when moonlighting is included is one of the most frequent and easily missed violations. This often happens because moonlighting hours—both internal and external—are tracked separately from the primary schedule, and the four-week average is not calculated prospectively. A compliant system must account for all clinical work from all sources as a single mathematical constraint.
How does Scheduling Wizard handle compliance for my specific subspecialty?
Scheduling Wizard handles subspecialty compliance by building your program's unique ACGME and institutional rules directly into its constraint-based scheduling engine. This goes beyond the Common Program Requirements. If you're in a surgical subspecialty with specific case logging needs or a neurology program with complex call structures, the rules that govern your schedule are treated as hard constraints, so the final schedule is 100% compliant for your specific program.
Does Scheduling Wizard replace our program's use of Amion or QGenda?
No, Scheduling Wizard complements and simplifies your use of tools like Amion or QGenda. It replaces the time-consuming and error-prone process of manually creating the block schedule. We deliver a finished, compliant, and optimized schedule in an Excel format that you can directly upload to your existing platform for daily viewing, paging, and communication.
How will the 2026 ACGME rule changes affect our scheduling?
The 2026 ACGME revisions, particularly counting at-home call towards the 80-hour weekly max and enforcing a 24-hour hard cap on continuous work, will make compliant scheduling significantly more complex. These new rules add more mathematical constraints that are difficult to manage with spreadsheets or manual tools. A constraint-based system like Scheduling Wizard is designed to adapt to these changes, incorporating the new rules into its logic to keep your program compliant.
What’s the difference between a tool that “audits” compliance versus one that “enforces” it?
A tool that "audits" compliance checks for violations after the schedule is built, forcing you into a painful cycle of manual fixes that can create new problems. A system like Scheduling Wizard that "enforces" compliance treats ACGME rules as unbreakable mathematical constraints from the start. This means it is impossible to generate a schedule that contains violations, eliminating the need for post-hoc audits and corrections.
How is an official "day off" defined by the ACGME?
An official day off is a continuous 24-hour period completely free from all clinical and academic responsibilities. A common mistake is counting the morning after a 24-hour call as a "day off." This is incorrect; that time is a required post-call rest period. ACGME rules mandate an average of one true day off per seven days when measured over a four-week block.
How can we prevent violations of the 16-hour shift limit for PGY-1s?
Preventing PGY-1 shift violations requires a scheduling system that treats interns as a distinct group with their own hard-coded rules. Using recycled templates or generic software often leads to this error. A compliant system must have the 16-hour cap for PGY-1s built-in as a non-negotiable constraint, automatically preventing them from being assigned to 24-hour calls or longer shifts.
How do you handle last-minute changes like sick calls?
While Scheduling Wizard delivers the master block schedule, real-time changes are typically managed by the program. However, because our schedules are built to be fair and balanced, finding appropriate backup coverage is often simpler. For major disruptions, programs can request a mid-block re-optimization to generate a new, fully compliant schedule for the remainder of the period, preventing the cascading violations that often result from manual patches.
Ready for a Schedule That Doesn't Need Auditing?
If your program is still building schedules in spreadsheets — or using software that flags violations after the fact — there's a better way.
Submit your program's constraints and see what a mathematically optimized, ACGME-compliant schedule looks like for your rotations, your residents, and your program requirements. No software to learn. No manual auditing required. Just a finished schedule that works.