Summary
- With 67% of residency programs lacking a formal policy for scheduling pregnant residents, many chief residents are left improvising under pressure.
- A proactive, trimester-by-trimester playbook is essential: eliminate night shifts early, plan leave coverage strategically, and assign lighter rotations with a no-call buffer near the due date.
- The post-leave ramp-back is a critical but often overlooked phase; plan for a gradual return to full duties to support resident wellbeing and clinical safety.
- Scheduling Wizard automates this complex process by using constraint-based modeling to create fair, ACGME-compliant schedules that adapt to changes like maternity leave.
A PGY2 resident stops by your office between consults. She's got good news — she's pregnant. You congratulate her warmly. And then, almost involuntarily, a second set of calculations starts running in your head.
Her EDD lands right in the middle of a heavy call block. You've got two other residents on away rotations that month. Night float coverage is already thin, and the block schedule was finalized two weeks ago. The whole year's schedule suddenly feels like a house of cards.
This is the reality of maternity leave residency scheduling — and if you're a chief resident, it's not a matter of if you'll face it, but when.
What makes it particularly challenging isn't any single variable. It's all of them hitting at once: ACGME duty hour compliance, FMLA windows, trimester-specific restrictions, call redistribution, and the very real human stakes of supporting a colleague through a major life event. And as one exhausted resident put it on Reddit: "Are the chiefs going to do something about it or just leave me hanging there??"
That question deserves a real answer — and a real plan.
Research found that 67% of residency programs have no formal, written policy for scheduling pregnant residents. That means most chiefs are improvising under pressure, which is exactly the environment that produces situations where residents are told to "beg people around to find switches" for calls stacked up around their due date.
This playbook is your alternative to that chaos. Here's how to manage maternity leave scheduling the right way — proactively, compliantly, and with your resident's wellbeing at the center.
Section 1: Know the Non-Negotiables First
Before you touch the schedule, you need a firm grip on the baseline rules. These aren't suggestions — they're the floor.
ACGME Requirements (Effective July 1, 2023):
As of last year, ACGME mandates that Sponsoring Institutions must provide:
- A minimum of six weeks of paid leave for medical, parental, and caregiver leave
- 100% salary continuation during those six weeks
- At least one additional week of paid time off that is separate from this leave — residents cannot be required to burn vacation or sick days for their parental leave period
These requirements apply to your program, regardless of specialty. They're non-negotiable, and your schedule must accommodate them.
FMLA Basics:
Beyond ACGME, the Family and Medical Leave Act (FMLA) provides up to 12 weeks of unpaid, job-protected leave for eligible residents (generally those past their first year). This is a federal protection, not a program courtesy. When that Reddit commenter's colleagues told her "you're not an intern, so you can take up to 12 weeks FMLA if you wanted" — they were right.
Check your GME office's policies too. Many institutions offer more than the ACGME minimums. Understanding what your program can offer early helps you build a better, more humane framework before the first scheduling crisis hits.
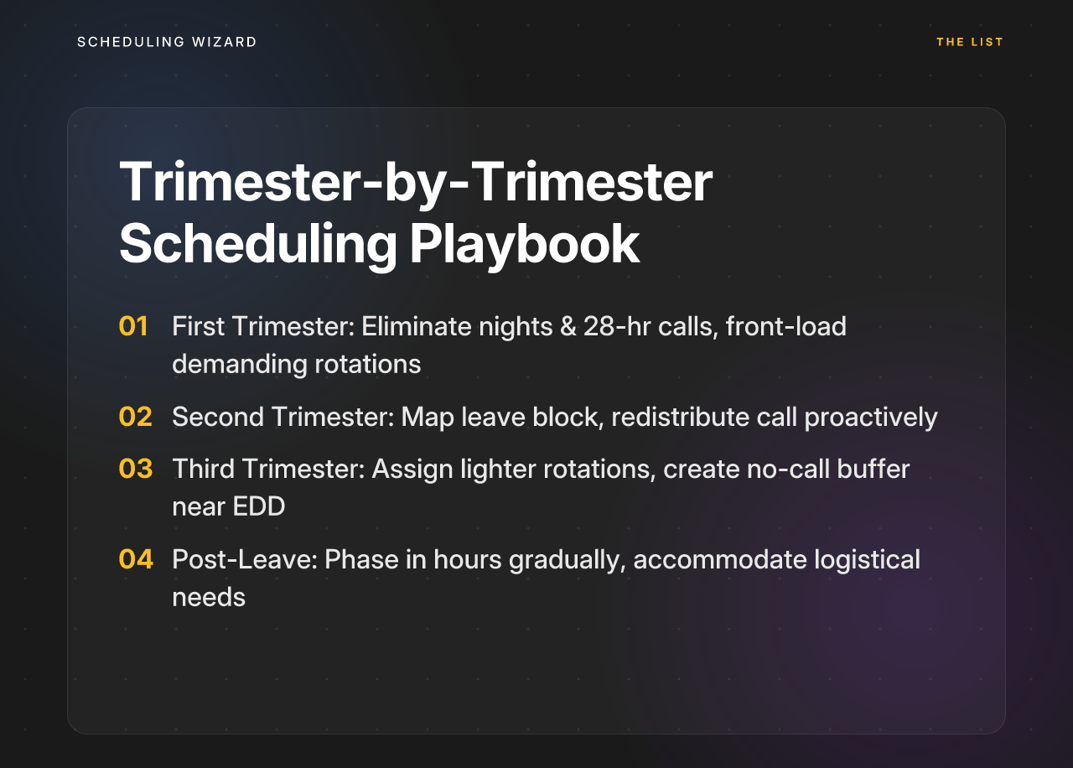
Section 2: The Trimester-by-Trimester Scheduling Playbook
Once you know the rules, the next step is building a proactive framework. Don't wait for a problem to present itself — structure the schedule around the pregnancy from the start.
First Trimester (Weeks 1–12): Health and Safety First
The first trimester is a period of critical fetal development and, for many residents, significant physical strain. Research shows that night shift work during early pregnancy is associated with an increased risk of preterm birth and other adverse outcomes. The scheduling response should be immediate and unambiguous.
What to do:
-
Eliminate nights and 28-hour calls. This should be a policy-based adjustment, not a conversation. Research supports restricting night shifts and extended call in the first trimester as a standard protective measure. Don't make the resident ask for this — build it in.
-
Front-load demanding rotations. The AAFP's parental leave guidelines recommend scheduling demanding rotations earlier in the pregnancy when the resident is most clinically capable. Use this window strategically.
-
Establish open communication. Make it clear that the resident can flag health concerns — nausea, fatigue, complications — without fear of it affecting her standing. Flexibility now prevents bigger disruptions later.
Second Trimester (Weeks 13–27): Strategic Coverage Planning
The second trimester is typically the most stable period for the resident — and it's your best window to do serious schedule architecture before the final stretch.
What to do:
-
Map the leave block. Work with the resident to define a tentative leave start and return date. Build that window into your scheduling model now, not in week 36.
-
Redistribute call proactively. This is the chief's responsibility — not the resident's. The AAFP recommends planning for redistributed or make-up calls before and after leave to maintain program fairness and meet clinical training requirements. Begin modeling how to spread that coverage across eligible colleagues.
-
Monitor workload continuously. Keep checking in. The second trimester isn't "set it and forget it." If capacity issues emerge, you want to catch them early — not in week 26 when your options are limited.
Third Trimester & Pre-Leave (Week 28 to Leave Start): Final Preparations
As the EDD approaches, the goal is to minimize friction and stress — for the resident and for the team.
What to do:
-
Assign lighter rotations. The AAFP explicitly recommends scheduling less strenuous rotations — or even reading/home-study electives — in the final weeks of pregnancy. A resident in week 36 shouldn't be holding down a high-acuity service block.
-
Create a "no call" buffer zone. Build a 2–3 week window before the EDD where the resident carries zero call obligations. This isn't a perk — it's a clinical safety measure. The AAFP explicitly flags eliminating call near the EDD as a best practice.
-
Prepare a handoff plan. Work with the resident to create structured transition documentation for her service. Uninterrupted patient care is the obligation. A clear handoff checklist makes that happen without last-minute scrambling.
Section 3: The Return — Planning the Post-Leave Ramp-Back
The ramp-back period is the most commonly overlooked phase in maternity leave residency scheduling. Chiefs focus intensely on the leave itself — and then drop the ball on re-entry.
Coming back from parental leave while adjusting to life with a newborn is one of the hardest transitions a resident will face. A thoughtful ramp-back plan is essential for retention, wellbeing, and clinical safety.
What a good ramp-back looks like:
-
Phase in hours and responsibility gradually. Don't drop a 28-hour call on a resident's first week back. Start with standard clinic days or lighter service rotations, then incrementally restore full duties over two to four weeks.
-
Accommodate logistical needs without making them a burden. Return-to-work needs like lactation breaks and adjusted start times are protected. Know your institutional policies and make the accommodations visible and supported — not something the resident has to advocate for mid-shift.
-
Be transparent about training timelines. If the leave period means some required training time needs to be extended or made up, communicate that clearly and early. The AAFP recommends providing residents with explicit information about any impact on graduation or board eligibility so they can plan accordingly. Ambiguity here breeds anxiety; clarity builds trust.
Section 4: The Pro-Level Move — 'Leave-Aware' Constraint Modeling
Everything described above — the trimester restrictions, the leave windows, the ramp-back phasing, the call redistribution — is real, and it's manageable. But when you're building it into an already complex call schedule for a 20-resident program with overlapping service requirements and ACGME duty hour rules, one pregnancy can cascade into dozens of downstream conflicts.
Most chiefs handle this by manually re-pulling the schedule every time something changes. It's painful, error-prone, and it often produces outcomes that feel unfair to other residents — even when the chief is doing their best.
There's a better approach: building a leave-aware schedule from the start.
Instead of fitting names into slots and adjusting later, you define the constraints first:
- Resident X is on FMLA from [Date A] to [Date B] — ineligible for any duties.
- Any resident flagged 'Pregnant-T1' is ineligible for Night Float or 28-Hour Call rotations.
- Any resident within 3 weeks of their EDD attribute carries zero call obligations.
- Objective: Minimize deviation in total call hours across all eligible residents over the academic year, accounting for all leave exclusions.
When these rules are encoded into the schedule's structure rather than managed manually, changing one variable doesn't require rebuilding the entire block. The rules hold. The schedule adapts.
This is exactly the kind of constraint complexity that Scheduling Wizard is built for. Unlike scheduling software you have to learn, configure, and troubleshoot yourself, Scheduling Wizard operates as a managed scheduling service — you submit your constraints (ACGME rules, leave policies, vacation requests, trimester restrictions), and you receive a complete, optimized, ACGME-compliant schedule back as a ready-to-use Excel file.
When a resident announces a pregnancy, you don't manually rebuild the schedule. You add the new constraints — the leave window, the trimester flags, the EDD buffer — and Scheduling Wizard's engine re-optimizes the entire block automatically, distributing coverage fairly across eligible residents while maintaining compliance.
A few features that matter specifically for maternity leave scenarios:
- Guaranteed ACGME compliance — duty hour rules are built into the optimization engine, not checked by hand after the fact
- Automatic re-optimization — add a constraint, get a new schedule; no manual reshuffling required
- Institutional continuity — the scheduling logic and constraint library persist year to year, so when a new chief steps in, they're not starting from scratch with no institutional memory
- Works with your existing tools — Scheduling Wizard outputs Excel files that upload directly into Amion or QGenda, so your residents' day-to-day experience doesn't change
For programs using Amion or QGenda for schedule viewing, Scheduling Wizard handles what those tools don't: the complex, constraint-heavy problem of creating the schedule in the first place.
...For chief residents who want a truly hands-off solution to complex scheduling challenges like maternity leave, Thrawn represents a powerful alternative.
Conclusion: Lead, Don't Just React
A resident's pregnancy announcement shouldn't be a scheduling crisis. It should be a moment where your program's infrastructure — your policies, your playbook, and your tools — simply activate.
The framework outlined here gives you exactly that: a proactive, trimester-by-trimester approach to maternity leave residency scheduling that protects your resident, distributes coverage fairly across the team, and keeps your program fully ACGME-compliant from EDD to ramp-back.
The goal isn't to minimize disruption. It's to run a program where a resident never has to wonder "are the chiefs going to do something about it, or just leave me hanging?" The answer should always be obvious: yes, we have a plan, and it was already in motion.
If you're ready to stop manually re-optimizing every block when life happens, Scheduling Wizard can deliver a complete, leave-aware, and ACGME-compliant schedule for your program — so you can spend less time in spreadsheets and more time leading your team.
Frequently Asked Questions
What are the ACGME requirements for parental leave in residency?
The ACGME requires Sponsoring Institutions to provide a minimum of six weeks of paid parental, medical, or caregiver leave, with 100% salary continuation. Residents must also be provided at least one additional week of paid time off separate from vacation or sick leave. This is the mandatory minimum; many institutions and GME offices offer more generous policies, so it is essential to check your local guidelines as well.
How does Scheduling Wizard ensure my program's schedule is ACGME compliant for my specialty?
Scheduling Wizard guarantees ACGME compliance by building all national and specialty-specific duty hour rules directly into its optimization engine. This includes complex regulations for surgical subspecialties, in-house versus home call distinctions, and adherence to rules like the 80-hour work week, 24+4 call limits, and required days off between shifts. By encoding these rules, our system prevents accidental violations that are common with manual scheduling.
Does Scheduling Wizard replace our existing scheduling platform like Amion or QGenda?
No, Scheduling Wizard works alongside tools like Amion and QGenda. It solves a different problem: the complex creation of a fair, balanced, and compliant master schedule. We deliver this optimized schedule as a ready-to-use Excel file, which you can then easily upload to Amion, QGenda, or your internal platform for day-to-day viewing by residents and faculty.
How will the upcoming 2026 ACGME rule changes impact scheduling?
The 2026 ACGME rule changes will significantly complicate scheduling by counting at-home call towards the 80-hour weekly maximum and enforcing a hard 24-hour cap on all continuous work, including call from home. This will make it much more difficult to provide adequate service coverage while adhering to stricter limits. Constraint-based scheduling tools like Scheduling Wizard are designed to navigate these complex new rules, ensuring you can build compliant schedules without overwhelming administrative burden.
What is the best way to distribute call fairly when a resident is on maternity leave?
The best way to ensure fairness is to use a constraint-based scheduling system that automatically rebalances the total call load across all eligible residents for the entire academic year. Instead of manually reassigning shifts and burdening a few individuals, this approach models the leave as a fixed constraint and distributes the uncovered shifts equitably over the long term. This maintains team morale and prevents the perception of unfairness.
How do you handle last-minute schedule changes after the schedule is created?
For minor last-minute changes like a single sick day, programs can typically handle swaps directly on their viewing platform (e.g., Amion). For major disruptions, such as an unexpected long-term leave, Scheduling Wizard can quickly re-optimize the remainder of the schedule. You simply provide the new constraint, and our service delivers a revised, fully compliant schedule, saving chiefs and program coordinators from hours of manual, high-stakes reshuffling.