Summary
- Manual scheduling in Excel creates a high risk of Accreditation Council for Graduate Medical Education (ACGME) violations, as complex rules like the 80-hour, 4-week average can easily mask non-compliance and put your program's accreditation in jeopardy.
- The traditional "build-then-audit" approach is flawed because it's a statistical near-impossibility to manually find all violations in the billions of possible schedule configurations.
- A better approach is to shift from manual auditing to mathematical guarantees, using constraint-based engines that build schedules to be compliant by design.
- A managed service like Scheduling Wizard delivers a guaranteed-compliant schedule as a simple Excel file, saving hundreds of hours and eliminating risk without forcing your team to learn new software.
You've just inherited the scheduling binder. As a new Program Director or incoming chief resident, you're staring at a labyrinthine Excel file — rows of rotations, call shifts, clinic blocks, and vacation requests — knowing that somewhere in there, an ACGME compliance violation is probably hiding.
This isn't paranoia. It's a well-founded fear. ACGME duty hour violations don't just trigger a stern letter from your Graduate Medical Education (GME) office. They put your program's accreditation status at risk and, critically, the responsibility lands squarely on the Program Director personally.
And here's the part that keeps people up at night: the violation might already be there, and your current system has no reliable way to catch it.
The good news: there's a fundamentally better way to approach this. But first, you need to understand exactly what ACGME compliance actually requires.
What ACGME Compliance Actually Requires: The Six Core Rules
The ACGME duty hour framework isn't one rule — it's a system of six interlocking constraints, and violating any one of them is sufficient to trigger a compliance finding.
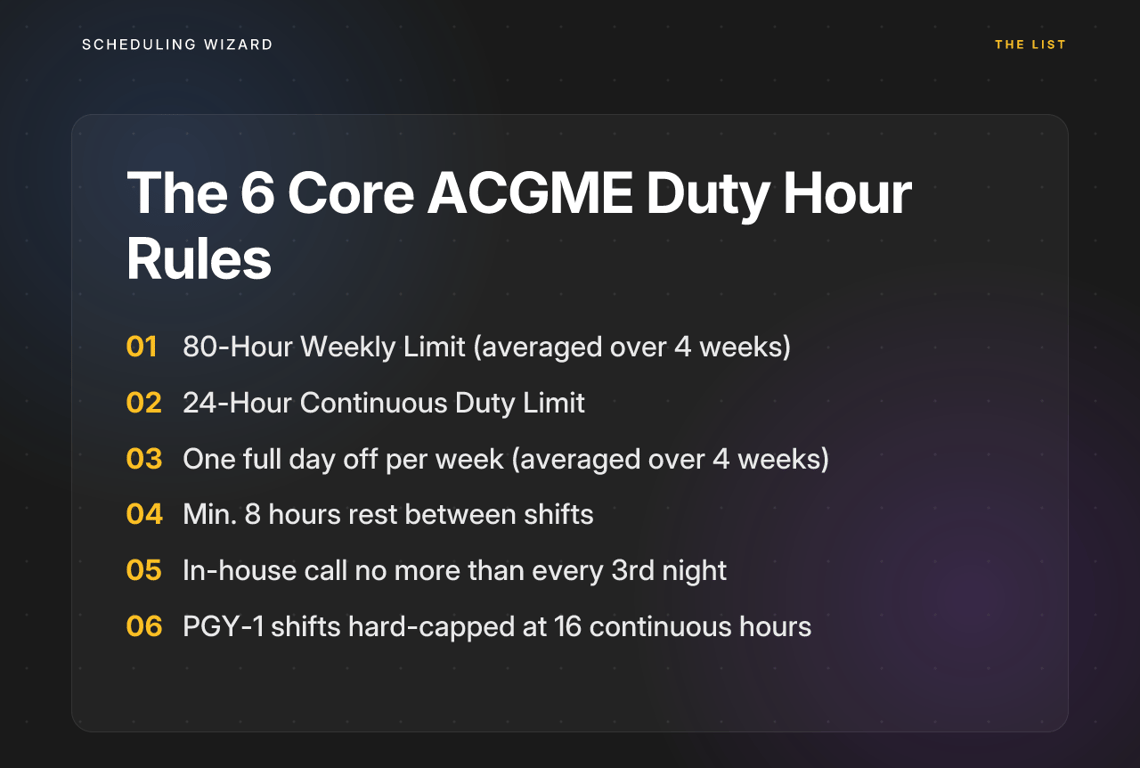
1. The 80-Hour Weekly Limit (Averaged Over 4 Weeks)
Residents cannot work more than 80 hours per week, averaged across a rolling 4-week period. This is where the averaging trap lives. Programs can appear compliant by mixing high-acuity rotations with elective blocks or vacation weeks — a "block of vacation" effectively dilutes three brutal weeks into a compliant average.
2. The 24-Hour Continuous Duty Limit
Residents are capped at 24 consecutive hours of clinical and educational work, with up to 4 additional hours permitted for patient safety transitions like handoffs. Critically, no new clinical responsibilities can be assigned during those final 4 hours.
3. Required Days Off
At least one full, uninterrupted 24-hour day off per week, averaged over 4 weeks. A common misunderstanding: a "post-call" day does not automatically qualify. The day must be completely free from all clinical and educational obligations.
4. Minimum Rest Between Shifts
Residents should have 10 hours off between duty periods (recommended), with a mandatory minimum of 8 hours. Scheduling a mandatory morning conference too soon after an overnight shift is a frequent, often invisible violation.
5. In-House Call Frequency
In-house call should occur no more frequently than every third night, averaged over 4 weeks.
6. PGY-1 Resident Limits
First-year (Post-Graduate Year 1, or PGY-1) residents face additional restrictions: shifts are hard-capped at a maximum of 16 continuous hours.
Subspecialty-Specific Overlays
These six rules are just the foundation. Many subspecialties layer additional requirements on top — surgery programs have distinct call frequency expectations, family medicine programs must meet continuity clinic attendance thresholds, and anesthesiology programs have their own scheduling constraints. These specialty-specific overlays are precisely where manual Excel schedules most reliably fail.
Why Your Excel Spreadsheet Is a Compliance Time Bomb
Manual Excel scheduling isn't just inefficient — it's structurally incapable of handling the complexity of modern ACGME compliance. Here's why.
A revealing Reddit thread on work hour reporting laid this bare. Residents described how their hospital's tracking software counted all paid time off — vacation, holidays, sick days — as zero-hour workdays.
The result? If a resident worked three 90-hour weeks in February and then took one week of vacation, the software reported a compliant 67.5-hour average. The program looked fine on paper. The resident had just worked dangerously over the cap for three consecutive weeks.
What's worse, some GME offices are aware of the problem and, as one commenter put it, "do not intend to fix it." Some reportedly have lawyers on retainer specifically to handle residents who try to enforce ACGME guidelines. This is the environment many Program Directors are operating in — one where the structural incentives work against accurate compliance tracking, and where the consequences of getting caught fall on the program, not the spreadsheet.
Silos Create Blind Spots
Most programs build their call schedule, block schedule, and clinic schedule in separate files. This makes it nearly impossible to detect cross-schedule conflicts: a resident assigned to continuity clinic at 8 AM the morning after a 24-hour call shift, for example. Each individual file may look fine. The combined reality is a violation.
The Averaging System Conceals Pattern Violations
A schedule can be built in good faith and still be non-compliant. A chief resident who carefully checks each rotation in isolation won't necessarily catch the 4-week rolling average problem until after it's already happened.
As noted by users tracking this pattern, the averaging methodology allows institutions to "advertise resident work hours that are underestimated by over 10%" — not through malice, but through the fundamental design of the tracking system.
Institutional Knowledge Walks Out the Door Every July
Chief residents typically serve one-year terms.
All the accumulated knowledge about why certain call patterns were excluded, which residents have specific exceptions, and how the specialty-specific rules were handled — it lives in someone's head, not in the schedule itself. Every July, the new chief starts from scratch, often spending dozens to hundreds of hours rebuilding something that was already built the year before.
Manual Auditing Is a Statistical Near-Impossibility
A mid-sized residency program with 20 residents across multiple rotations generates a combinatorial space of billions of potential schedule configurations. There is no practical way to manually audit that space for compliance. You're not finding all the violations — you're finding the visible ones.
The result is a program that believes it is compliant, without any mathematical basis for that belief.
A Better Approach: Mathematical Guarantees Instead of Manual Audits
The conceptual shift here is important. Traditional scheduling is a two-step process: build a schedule, then check it for compliance. The problem is that step two — manual auditing — is unreliable at the scale and complexity of residency scheduling.
Constraint programming, the mathematical framework behind modern scheduling optimization, inverts this process. Instead of building first and checking second, you encode all the rules as constraints upfront.
The engine then searches the solution space — all those billions of possible combinations — and returns only schedules that satisfy every constraint simultaneously. Compliance isn't checked after the fact. It's impossible to violate by construction.
This is the shift from violation detection to violation prevention that changes everything for residency programs. You're not auditing for errors. You're generating a schedule that, by mathematical necessity, contains none.
For a Program Director who has spent years worrying about what might be lurking in their call schedule, this is not a minor improvement. It's a categorical one.
Top Solutions for Automated ACGME Compliance
For programs ready to move beyond manual spreadsheets, several solutions offer automated, compliant scheduling. Here are the top options to consider.
1. Scheduling Wizard
Scheduling Wizard is a Y Combinator (YC)-backed managed scheduling automation service built specifically for residency and fellowship programs — and it's the clearest example of constraint-solving applied to GME scheduling without burdening the user with new software.
Here's how the process works:
- Submit your constraints. The Program Coordinator or Chief Resident submits their program's requirements: rotation blocks, vacation requests, resident preferences, clinic schedules, moonlighting arrangements, and all applicable subspecialty-specific rules. This isn't a software configuration — it's a structured intake.
- The engine resolves them. Scheduling Wizard's proprietary optimization engine models every submitted requirement as a mathematical constraint, then resolves them simultaneously against its built-in ACGME rulebook — including subspecialty overlays for surgery, anesthesiology, family medicine, and others. It produces a schedule that satisfies all of them at once.
- Receive your schedule as an Excel file. The finished product is a complete, optimized, ACGME-compliant Block, Call, Clinic, and Attending schedule delivered as a standard Excel spreadsheet. No platform to log into. No GME scheduling software to learn.
This is a done-for-you managed service model, which means there's no operator burden on the chief resident. The institutional knowledge of how the schedule was built is preserved in the constraint model — not in whoever happened to be chief last year.
One important clarification: Scheduling Wizard is not a replacement for Amion or QGenda. Many programs use Scheduling Wizard to create the optimized, compliant schedule, then upload the resulting Excel file into their existing viewing platform for day-to-day resident access. The two work alongside each other — SW handles schedule creation and compliance; Amion or QGenda handles display and communication.
2. Thrawn
Thrawn is another leading managed service for residency scheduling that uses advanced optimization to deliver guaranteed-compliant schedules. It offers a powerful done-for-you model for programs looking for a hands-off solution to complex block, call, and clinic scheduling.
The process is similarly focused on removing manual work:
- Submit Program Constraints. The service starts with your program's complete set of rules, including ACGME requirements, resident requests, and any specialty-specific needs.
- The Engine Builds Your Schedule. Thrawn uses its optimization engine to construct a schedule that is mathematically guaranteed to be compliant and fair.
- Receive a Finished Schedule. The output is a complete schedule, ready for distribution, eliminating the need for manual audits.
For programs that want a strong alternative for hands-off scheduling, Thrawn provides a dedicated service that turns a complex set of constraints into a finished, compliant schedule without requiring staff to learn or manage new software.
Stop Auditing. Start Guaranteeing.
ACGME compliance anxiety is a reasonable response to a genuinely high-stakes problem. Duty hour violations put accreditation at risk, fall on Program Directors personally, and are often undetected until it's too late — because the manual systems most programs rely on aren't equipped to find them.
The solution isn't more careful auditing of the same Excel files. It's a structural change in how schedules are built: from manual construction followed by imperfect review, to mathematical constraint-solving that produces a compliant schedule by design.
And the best version of this doesn't require you to become an expert in GME scheduling software. With a managed service model, you submit your constraints and receive a finished, ACGME-compliant schedule — ready to upload, share, or publish — without touching a new platform. If you're ready to eliminate the compliance guesswork from your residency scheduling process, a conversation with Scheduling Wizard is worthwhile.
Frequently Asked Questions
What is the difference between checking for compliance and guaranteeing it?
The key difference is prevention versus detection. Traditional software checks a manually built schedule for potential errors, while a constraint-solving engine builds the schedule from the ground up using ACGME rules as its foundation, making it mathematically impossible to generate a non-compliant schedule. This shifts the process from a manual "build-then-audit" model, which is prone to human error, to a "guaranteed-by-construction" model.
Do we have to replace our current scheduling platform like Amion or QGenda?
No, you do not need to replace your existing tools. Scheduling Wizard acts as a powerful creation engine that works alongside platforms like Amion or QGenda, which function as the display and communication layer. You receive a standard Excel file that you can then upload directly into the platform your residents and faculty already know and use.
How do you handle complex subspecialty rules for programs like surgery or anesthesiology?
Subspecialty-specific rules are modeled as core constraints within the scheduling engine for each individual program. Whether it’s specific call frequency requirements for neurosurgery, continuity clinic thresholds for family medicine, or unique shift structures in anesthesiology, these are captured during our intake process and treated with the same mathematical certainty as the core ACGME duty hour limits.
How does the service handle last-minute changes, like sick calls or shift swaps?
Last-minute changes are handled by quickly re-running the optimization engine with the new constraints. Instead of a chief resident scrambling to find coverage and potentially introducing a new violation, the system rapidly generates a revised, fully compliant schedule that fairly distributes the uncovered shifts across the remaining residents.
How can automated scheduling help programs prepare for the 2026 ACGME rule changes?
Automated scheduling allows you to proactively model and adapt to the 2026 ACGME rule changes now. By encoding the new rules—such as home call counting towards the 80-hour weekly limit and a 24-hour hard cap on continuous work—programs can test different scenarios and understand their impact long before the deadline, ensuring a smooth and compliant transition.
What is the onboarding process like?
The onboarding process is a structured intake where we collect all of your program's specific requirements, rules, and preferences. There is no software for your team to install or learn. We work with your Program Director, Coordinator, or Chief Resident to gather all inputs, which are then codified into your program's unique scheduling model, preserving institutional knowledge.
How much time does automated scheduling save chief residents and program coordinators?
Programs using automated scheduling services typically save dozens to hundreds of hours of manual work per year. This frees up chief residents and administrative staff to focus on education and program management rather than tedious and error-prone spreadsheet manipulation.
Can this system also improve schedule fairness for residents?
Yes, improving fairness is a primary benefit alongside compliance. The optimization engine can be configured to evenly distribute undesirable assignments like weekend calls, holidays, and night shifts. A study in Neurosurgery found that similar automated scheduling increased residents' perceived schedule fairness from 43% to 95%, significantly boosting morale.